
On November 13th, the PUMCH rheumatology team published original findings on medication discontinuation in stable systemic lupus erythematosus (SLE) patients online in Annals of the Rheumatic Diseases (IF: 20.3), a leading rheumatology journal. Led by Chief Physician Fei Yunyun, Executive Deputy Director of the Department of Health Management and rheumatology specialist, and Deputy Chief Physician Zhao Lidan, the nationwide multicenter randomized controlled trial showed that approximately 70% of patients remained stable for six months after either discontinuing glucocorticoids (GC) alone or withdrawing all medications, though the latter approach carried an overall higher risk of relapse. Notably, hydroxychloroquine (HCQ) proved effective in preventing flares and sustaining remission after GC discontinuation. This research was funded by the National High Level Hospital Clinical Research Funding.
SLE is an autoimmune disease characterized by complex clinical manifestations and significant morbidity and mortality. Growing clinical experience and advances in medical technology now allow better control of SLE, though the disease remains incurable and requires long-term maintenance therapy. GCs play a key role in achieving and maintaining disease remission, and out of concerns about disease flares, most patients with stable SLE continue long-term low-dose GC maintenance therapy. However, extended GC treatment brings numerous side effects and complications, including potential organ damage.
For stable SLE patients, finding the right balance between preventing flares and minimizing GC side effects remains a critical challenge. Can stable SLE patients discontinue GCs? What are the relapse risks after withdrawal? What maintenance strategies are effective after GC discontinuation? The research team conducted this clinical study to provide high-level evidence-based answers.
The team led an investigator-initiated, prospective, non-inferiority design, randomized controlled trial across multiple centers in China. The study enrolled 333 stable SLE patients who had been maintained on low-dose GCs plus HCQ therapy with sustained stability for at least one year. Patients were randomized into three groups: drug-free (both GC and HCQ withdrawal management), HCQ (discontinued GC but maintained HCQ dosage), and dual maintenance group (both GC and HCQ continued without change). The study compared relapse rates between the groups after 33 weeks of follow-up.
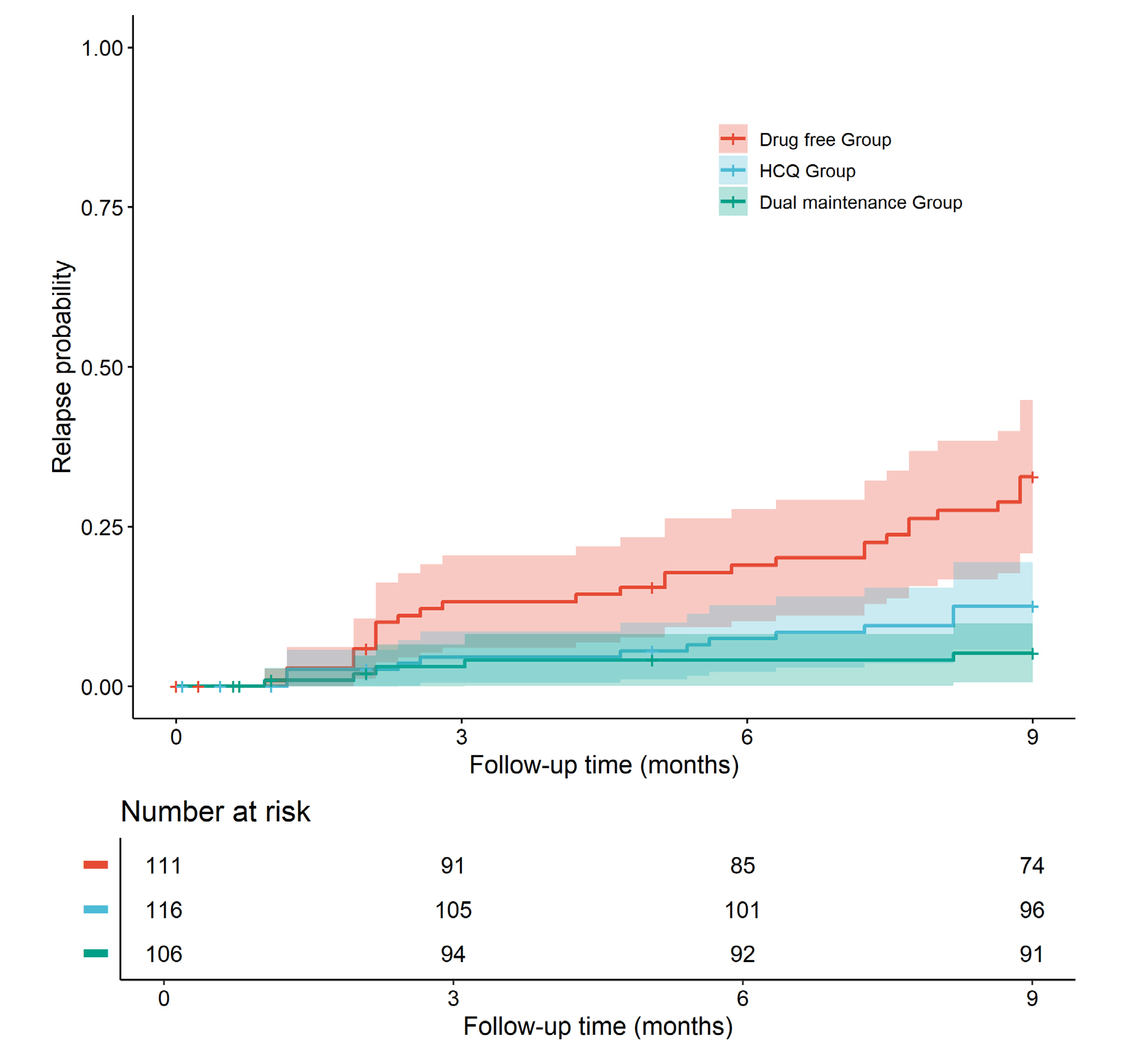
Results showed relapse rates of 26.1%, 11.2%, and 4.7% in the drug-free, HCQ, and dual maintenance groups, respectively. The drug-free group showed higher overall relapse risk compared to the dual maintenance group, while the HCQ group exhibited fewer flares after GC withdrawal than the drug-free group and achieved noninferiority in the relapse rate as compared with dual maintenance group. These findings suggest that GC discontinuation is feasible in stable SLE patients, with HCQ providing protective effects and reducing relapse risk, making it a suitable maintenance therapy option.
This study is the first international randomized controlled trial examining GC withdrawal and subsequent maintenance strategies in stable SLE, providing high-quality evidence for clinical practices. The study boosts confidence in GC-free maintenance and demonstrates HCQ's continued effectiveness in this context. According to Dr. Fei Yunyun, the team plans to further investigate the possibility of long-term GC discontinuation and identify characteristics of high-risk patients for post-withdrawal relapse.
Link to the publication:
https://ard.bmj.com/content/early/2024/11/13/ard-2024-225826
Written by Huang Sicheng
Edited by Fu Tanping