
Recently, a study led by Professor Xiao Yi’s team from the Department of General Surgery at PUMCH found that for patients with primary right-sided colon cancer without distant metastasis, the conventional standard D2 dissection is sufficient. For patients with suspected lymph node metastasis in the mesentery, the complete mesocolic excision (CME) with greater extent of dissection may generate more survival benefits. This research was published as an original article in the internationally prestigious Journal of Clinical Oncology (IF=42.1), providing high-level evidence-based guidance for precise surgical selection. It is the world’s first large-scale randomized controlled trial to demonstrate the safety and effectiveness of lymphadenectomy of different extents for right-sided colon cancer.
For treating right-sided colon cancer, the conventional D2 dissection only removes lymph nodes distributed around the tumor-containing colon segment and main blood supply arteries. In 2009, the complete mesocolic excision (CME) technique, as extended lymphadenectomy, was proposed. CME involves completely removing the cancerous colon and surrounding mesentery, ensuring the removal of all lymph nodes around the cancerous lesions. This approach helps reduce the risk of local recurrence and distant metastasis and improves patient prognosis. However, extended lymphadenectomy may also increase the occurrence of complications and cause damage to patients. When CME was first proposed, it was not backed up with high-level evidence.
Does extended lymphadenectomy provide more survival benefits for patients with right-sided colon cancer? To find out the answer, in 2016, Professor Xiao Yi’s team from the Department of General Surgery at PUMCH, in collaboration with methodological and gastrointestinal surgery experts, initiated a randomized controlled study: the Radical Extent of lympadenectomy: D2 dissection versus complete mesocolic excision of LAparoscopic Right Colectomy for right-sided colon cancer (RELARC) study. The RELARC study enrolled 1,072 adult patients diagnosed with primary right-sided colon cancer without distant metastasis from 17 Tertiary Grade A hospitals nationwide. By the end of 2019, the study completed the enrollment, assigning 536 patients to CME and 536 to D2 dissection. In early 2023, the research team completed 3-year post-operative follow-ups for all patients. There was no statistically significant difference in the 3-year disease-free survival (no recurrence, metastasis, or death) and overall survival between the two groups.
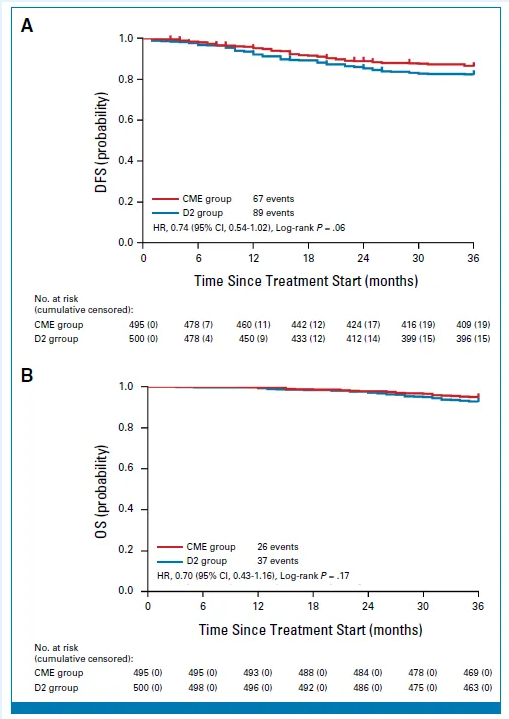
▲Comparison of 3-year disease-free survival (Figure A) and of overall survival (Figure B) between the 495 patients who underwent CME and the 500 patients who underwent D2 dissection. 77 patients were excluded from the study for various reasons
The study results show that for patients with primary right-sided colon cancer, standard D2 dissection is a safe and effective choice. For patients with suspected lymph node metastasis in certain areas, CME may provide better survival benefits. Compared with standard D2 dissection, CME does not increase the incidence of intraoperative and postoperative complications but does increase the risk of intraoperative vascular injury.
Professor Xiao Yi explained: “The RELARC study is notable for its large scale, extended duration, and involvement of multiple teams across the country. Its timely completion to a high standard showcases the dedication of Chinese colorectal surgeons to overcoming challenges through collaborative research. We hope this success will inspire our colleagues to engage in clinical studies with greater confidence and enthusiasm.” Moving forward, the team will disseminate these findings nationwide with the goals of promoting more precise selections of surgical techniques and preventing overtreatment, ultimately improving patient outcomes.
Written by Lu Junyang and Gan Dingzhu