
A research team led by Director Zheng Jun and Deputy Director Zhang Chaoji of the Department of Cardiac Surgery at PUMCH recently published a clinical study in the Journal of the American Heart Association (JAHA, a tier 1 journal ranked among the top 5% by the Chinese Academy of Sciences). The study provides high-level evidence-based guidance on surgical timing and valve strategy for patients with infective endocarditis (IE) combined with neurological complications, resolving a long-standing clinical dilemma and offering high-quality evidence to inform the management of high-risk patients worldwide.
With population aging and the increasing use of cardiac implant procedures, the incidence of IE has been rising. Approximately 20%–40% of patients with IE develop neurological complications, with mortality rates as high as 45%. For IE patients with neurological complications who meet surgical indications, surgery remains an effective treatment. However, clinicians face a therapeutic dilemma: cardiac surgery can directly remove the source of infection, but heparinization during cardiopulmonary bypass may worsen intracranial injury; delaying surgery can protect the brain, but increases the risk of spreading infection, worsening heart failure, and recurrent embolism that can become life-threatening. For IE patients with neurological complications, evidence to guide the optimal timing and type of surgery needed has long been lacking.
This retrospective cohort study included 663 patients with left-sided IE who underwent cardiac surgery at PUMCH between December 2012 and December 2024. Of these, 204 patients had preoperative neurological complications, including cerebral embolism, intracerebral hemorrhage, brain abscess, and infectious intracranial aneurysm.
Regarding surgical timing, the study found that in IE patients who had experienced cerebral infarction without hemorrhagic transformation, prompt surgery did not increase the risk of death. Among patients who developed intracerebral hemorrhage following cerebral infarction, surgery performed within 7 days carried a significantly elevated risk, whereas surgery performed at around 14 days was associated with a marked reduction in risk that subsequently leveled off. In terms of surgical decision-making, bioprosthetic valves have a lower anticoagulation intensity, effectively reducing the risk of intracranial hemorrhage and making them better suited to IE patients with neurological complications.
The study further revealed that peripheral vascular disease, mitral valve infective endocarditis, and S. aureus infection were independently associated with increased risks for IE patients with neurological complications, underscoring the need for comprehensive evaluation of such patients in clinical practice.
Traditionally, cardiac surgery and neurological care have been managed as separate and competing priorities, placing clinicians in a difficult position. The team led by Director Zheng Jun and Deputy Director Zhang Chaoji of the Department of Cardiac Surgery at PUMCH has advanced an integrated cardiac-neurological treatment framework and developed a five-tier risk stratification system — bringing mortality among IE patients with neurological complications down to 8.8%, with over 80% of those with concurrent brain injury achieving favorable neurological outcomes after surgery.
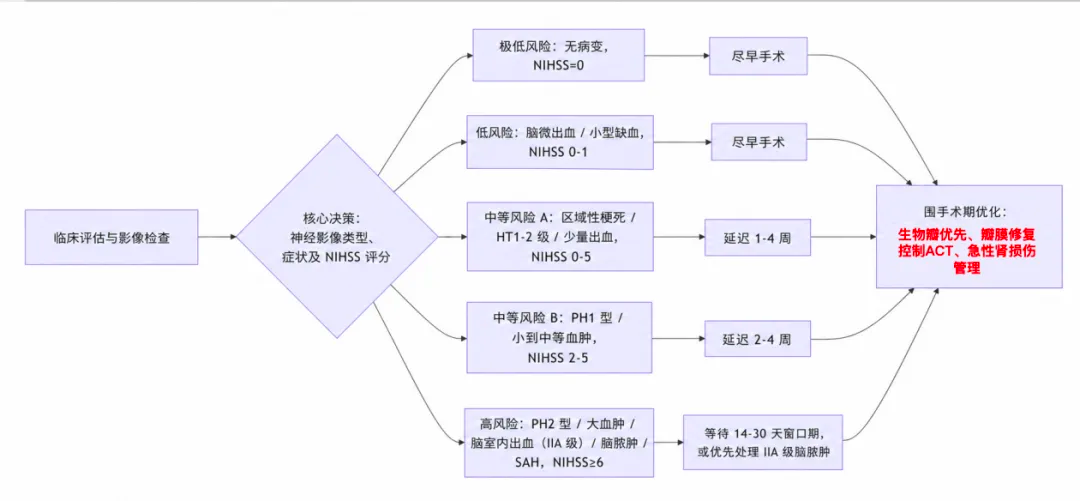
▲Decision diagram of the five-tier risk stratification system for infective endocarditis patients with neurological complications (HT: hemorrhagic transformation; PH: parenchymal hematoma following cerebral infarction; IIA: infectious intracranial aneurysm; SAH: subarachnoid hemorrhage; NIHSS: National Institutes of Health Stroke Scale)